Archives
If you didn’t read this great round-up of how the House AHCA and the Senate BCRA would increase the uninsured, cut Medicaid, and affect Texas, go take a look now. With the July 4th holiday, you may have missed a couple of updates adding to the growing body of evidence of deep harm to our most vulnerable Texans and to hard-working families threatened by both of these bills.
Because the Senate bill included an old legislative trick—delaying a big Medicaid cut to the end of the decade to camouflage its impact—members of the Senate Budget and Finance committees requested a supplemental CBO report on the long-term effects (i.e., the impact over the second decade of the proposed law) of the Senate health care bill’s Medicaid growth cap. The CBO published that analysis last week (6/29), and that report shows that while national Medicaid spending would be cut to 26 percent lower in 2026 than it would be under current law, the deeper cuts cause the reduction to the Medicaid to grow to 35 percent in 2036.
The next day (6/30), some new estimates of the 50-state impact of the Senate bill were released by Manatt Health, for the Robert Wood Johnson Foundation. The authors report that the 19 non-Medicaid expansion states are still slated to lose $53 billion from 2020 to 2026 in federal Medicaid dollars because of the per capita cap that launches in 2020. Cuts to the existing (pre-ACA expansion) Medicaid program will hit people with disabilities the hardest, with seniors, children, and pregnant women following behind.
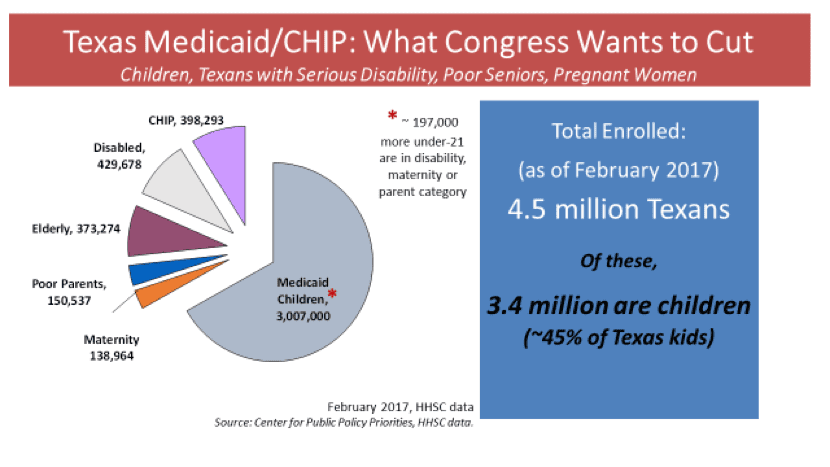
The analysts predict Texas would lose $10.5 billion in federal Medicaid dollars for our current (unexpanded) Medicaid program between 2020 and 2026. That’s about $1.5 billion a year.
Of this loss, $4 billion would be for care for Texans with disabilities, $2 billion for seniors, $3.4 billion for children, and $1 billion for pregnant women and the small number of parents who qualify for Texas Medicaid.
Our Texas Legislature recently opted not to invest $75 million a year to reverse damaging cuts to pediatric Medicaid payments for speech, physical, and occupational therapy. A loss of federal Medicaid funds of $1.5 billion a year is unlikely to be replaced by our current leadership, and the injury will be borne by our most vulnerable Texans.

CPPP Senior Policy Analyst Stacey Pogue co-wrote this post.
It is unclear when the U.S. Senate will vote on its Medicaid cut and repeal of the Affordable Care Act (ACA) bill, the “Better Care Reconciliation Act” (BCRA). CPPP will keep posting updates, and it’s important to keep urging Senators to oppose this scheme.
The non-partisan Congressional Budget Office has released its detailed “score” for the BCRA. The CBO analysis confirms that the bill is in some critical ways even more damaging to health care than the U.S. House’s “American Health Care Act.”
Though the Senate bill’s authors claim they intend to improve U.S. health care, the bill is projected to result in millions more uninsured Americans. Some 15 million more would be uninsured right away in 2018, building to 22 million more uninsured in 2026. By 2026, the scheme would reduce U.S. Medicaid enrollment by 16 percent, leaving 15 million fewer Americans covered by Medicaid, including cuts to Medicaid in non-Medicaid-expansion states like Texas.
As we have noted, the big-picture problems in the Senate bill (BCRA) include:
- Cut Texas Medicaid deeply—perhaps even more than the House bill. The bill includes deep cuts to the “traditional” Medicaid program that Texas has, not just the ACA Medicaid Expansion (and the cuts get much deeper in 2025).
- Makes insurance less affordable, not more, for millions with private insurance by increasing premiums and deductibles, while hitting consumers age 40 and older hardest.
- Uses the Medicaid and subsidy cuts to pay for tax cuts for big corporations and high-income households.
- Offers zero help to lower premiums or deductibles for middle-income families getting little or no subsidy today. Nothing is done to help the majority of Texans who are covered through employment with their high costs (in fact, makes things worse for Texans asked to pay a high share on employer coverage).
This should be reason enough to call your Senators and tell them to oppose the Senate health care scheme. But read on to find out more.

The Texas Senate and House of Representatives have agreed on a $217 billion 2018-2019 budget, officially named Senate Bill 1. Eva DeLuna Castro has a good overview of the whole budget. Let’s take a closer look at the funding for Medicaid.
Total funding for Medicaid in 2018-2019 is $62.4 billion All Funds ($26.3 billion non-federal).
- This is actually lower than the amounts allocated and spent for the current 2016-2017 budget (that is, the 2015 appropriations plus the supplemental appropriation to finish out 2017).
- The largest Medicaid budget cut directive is in Health and Human Services (HHSC) Rider #34 Cost Containment, which requires the agency to reduce Medicaid spending by $830 million All Funds ($350 million General Revenue).
- HHSC Rider #158 requires savings from a less generous formula used to set Medicaid Managed Care premium rates: $182.6 million All Funds ($76.3 million GR).
The budget covers what the Legislative Budget Board (LBB) estimates for caseload growth for Medicaid for 2018, but NOT for 2019; also unfunded is projected cost growth per Medicaid participant for 2018 or 2019. The LBB has not released recent projections of these unfunded amounts. Early in the session, Medicaid caseload growth for the full biennium was scored at over $700 million GR, so shorting the budget for just one year can be estimated around $300 million GR. HHSC has estimated the amount of the cost/inflation needs as high as $1.9 billion GR; so with updates and lower LBB assumptions, the gap between this appropriation and the need for 2018-2019 could range from $1.2 to $1.5 billion GR.
SB 1 only restores 25 percent of the Medicaid pediatric therapy rate cuts mandated in the 2016-2017 budget. The House version of SB 1 included a 75 percent restoration of the therapy rates, and the House version of HB 2 the supplemental bill included funds for 2017 restoration and a repeal of the directive for HHSC to move ahead seeking additional cuts; none of these positive proposals survived.
SB 1 includes funding for 735 Promoting Independence waiver “slots”, and another 276 for children in Child Protective Services custody who need long-term services and supports. Rate cuts to some community care waiver providers and inadequate wages for personal attendant who care for Medicaid’s clients with disabilities and seniors are not addressed in the budget.
How big is that can we are kicking down the road? This Medicaid “IOU” is not as big as the 2011 session’s IOU, which was nearly $5 billion GR when they passed their budget. As noted above, there is no recent official public LBB scoring of the value of the unfunded Medicaid cost inflation for 2018-2019. But based on HHSC’s Exceptional Item requests, it is expected to fall between $1 billion and $1.5 billion GR. And, program reductions or efficiencies mandated in the riders described above assume another $426 million GR can be squeezed out of the already-lean program.
Lawmakers should expect to fill at least a $1 billion GR Medicaid hole in the 2019 session, and possibly closer to $2 billion if the costs run high and cost containment wish-lists cannot yield the required savings.
Stay tuned for more analysis of the Texas budget as details emerge.

Putting House and Senate Budget Cuts in Perspective
Eva DeLuna Castro’s Comparison of the Texas Senate and House Budgets includes some of the high-level concerns about the major gaps in both chambers’ Medicaid-Children’s Health Insurance Program (CHIP) proposals. This post and a new linked detailed table provides more details on Medicaid-CHIP, with special focus on Texans with disabilities and on children. But before we dive in, let’s look back at how funding has failed to meet 2017 needs. Let’s look at the impacts of tax breaks, revenue diversions and the talk in Congress of capping Medicaid funds for states. All these factors play into the real state of Texas Medicaid and its ability to continue to serve over 4 million Texans.
Both House and Senate Budget Bills Risk Cuts As Bad as 2003, 2011
And New State Revenue Cuts, Federal Medicaid Cap Proposals Could Force More Cuts in Eligibility, Benefits, and Provider Pay
REVENUE MATTERS. At some point Texas legislators will pass a balanced budget, but decisions they made in 2013 and 2015 to give tax breaks and divert revenue resulted in having $10 billion less to work with for the 2018-2019 budget. This shortage is independent of any lower revenues Texas has because of lower oil and gas prices. In addition to coming into this 2017 session without enough money, the Legislature is looking to pass another huge tax break – even considering eliminating Texas’ main business tax completely – which could send us into our 2019 session another $3.5 billion in the hole.
CONGRESS CONTEMPLATING REDUCING FEDERAL MEDICAID DOLLARS, TOO. All versions of the recent Obamacare Repeal bills have proposed reducing Congress’ federal funding to states for Medicaid. Therefore we cannot count on federal funds to prevent Medicaid cuts if our own state budget comes up short.
Current Medicaid Proposals Compare in Scope to Cuts in 2003, 2011:
We calculated total reductions for earlier budget periods and compared them to the actual “client-service spending” that the state of Texas reported to federal Medicaid authorities for those years (i.e., does not include administration costs or special supplemental payments). For 2018-2019, we used Texas HHSC’s current Medicaid projection for 2018 and inflated that amount by the recent average annual growth rate to model 2019.
2003: Sweeping Medicaid and CHIP cuts originally passed at nearly $1 billion of General Revenue (GR). Then Congress made recession-related relief dollars available, and the Legislative Budget Board (LBB) reduced cuts to 10.4 percent of client services.
2011: The Legislature passed direct cuts to Medicaid that were 10.5 percent of the actual client service spending for 2012-2013, a comparable percentage to 2003. In addition, the Legislature left roughly $4.5 billion GR as an explicit “IOU” for Medicaid, to be funded in the 2013 session supplemental bill. This IOU left Medicaid four to five months short of covering the full 24 months in the biennium, and the Legislature passed a supplemental appropriations bill early in the 2013 session to prevent default on payments for health care and long-term care. The 2011 rate and benefit cuts largely remained, however.
2017: As the small chart above and the detailed table below describe in detail, the House and Senate appropriations bills include a mixture of potential cuts and IOUs for Medicaid. Should all of the under-funding of Medicaid be achieved through program cuts—that is, if the 2019 Legislature cannot or will not fund the supplemental needs—then the total tally would be about 13 percent of projected Medicaid direct client services for 2018-2019. Because of this, the Legislature’s intentions and its ability to find revenue in 2019 are of paramount importance.
Remember: Texas Can’t Kick Medicaid Can down the Road, unless there will be Revenue Available down the Road.
To assess the threat to ongoing Texas Medicaid services for over 4 million Texas children, seniors, people with disabilities, and pregnant women, it is important to watch the House and Senate budget bills closely. But we also have to watch how the chambers have handled the current 2017 Medicaid funding shortfall, actions they’re taking with respect to using available dollars, and making sure adequate dollars will be available in the future.
- The Texas Senate has not yet passed a supplemental appropriations bill to fill the current Texas Medicaid shortfall for 2017 (and other key state budget needs for 2017). The House did pass its supplemental bill, which included $930 million state dollars for Medicaid in 2017.
- The House approved use of some funding from the Rainy Day Fund, and the Senate has not (the RDF is projected to have $12 billion available by the end of 2019).
- The House has included text expressing its intention not to make Medicaid program cuts in association with its “federal flexibility” rider that pulls $1 billion state GR dollars from Medicaid. However, other House Medicaid funding reductions do not come with those reassurances. The Senate has remained silent about its intentions.
Now, be sure to read our policy brief for some of our top concerns on the House and Senate budget proposals being considered by the state budget conferees.
The House Committee on Appropriations approved its budget proposal on March 29, and a floor vote by the full House is set for April 6. The bill will, as usual, undergo some additional amendments on the House floor. Let’s explore some key Medicaid and Children’s Health Insurance Program (CHIP) provisions in the House Committee bill. After the House finalizes its budget proposal CPPP will post a comparison of the House and Senate budget proposals on Medicaid-CHIP policy and funding..
Key takeaway: some aspects of the House Committee‘s $63.2 billion All Funds proposal for Medicaid are positive, but other provisions raise serious worries about the security of medical and long-term care for millions of Texans.
As we have noted elsewhere, in this 2017 session it is especially critical to consider the supplemental appropriations bills for the current 2016-2017 budget period as part and parcel of the 2018-2019 budget plans. Without considering supplemental appropriations, any analysis of funding for state services and use of revenues will have major gaps.
As Eva DeLuna Castro noted in her post before the House Committee vote on its 2018-2019 bill, HB 2, the House’s supplemental bill for 2017, would use $931 million in General Revenue (GR) for Medicaid, which would also bring Texas $1.7 billion in federal matching funds. Combined, this $2.6 billion would ensure that Texas can pay the health care costs of about 4.1 million low-income Texans through the end of August 2017. This gap in funding is largely the result of 2015 budget writers’ choice to leave projected Medicaid cost inflation out of the 2016-17 appropriations act. HB 2 would also provide funding or transfer authority in fiscal year 2017 to undo half of the 2015 Legislature’s cuts to Medicaid acute care therapy services ($51.3 million in state and federal funds).
So under the House Committee’s budget plan, Medicaid makes it out of the current 2016-2017 budget period in fairly good shape. For 2018-2019, the House Committee’s bill funds enrollment growth in Medicaid, but does not fund the Health and Human Services Commission (HHSC) “Exceptional Item” request for cost growth in Medicaid (scored at over $1.75 billion GR early in session).
But the 2018-2019 House proposal also includes some large-scale provisions that create significant questions and concerns. In order of size, they are:
- HHSC Rider 36: Medicaid Funding Reduction and Cost Containment. Since 2011, each state budget bill has included a Medicaid Cost Containment rider directing reductions in spending and listing a number of policy options for cutting that spending. The House bill calls for cutting total 2018-2019 Medicaid spending by $111 million of GR ($244 million of All Funds), and lists 15 options for pursuing savings, plus authority for the agency to identify other approaches. The Senate’s bill has a version of this rider that cuts several times as much; stay tuned for that update.
- Article IX Rider 17.10: Contract Cost Containment. This lengthy rider in Article IX of the bill calls for $496.3 million in spending reductions attributed to sweeping changes in contracting practices across all agencies, but over 90 percent of the reduction ($450.2 million) is directed to HHSC. Contracting practices and irregularities have come under intense scrutiny in recent years, with recommended changes coming from the Legislative Budget Board staff report, a state auditor’s report on HealthSpring (a Medicaid Managed Care StarPlus contractor), an HHSC report to the legislature, and a House Appropriations subcommittee on budget transparency.
- HHSC Rider 186: Federal Flexibility. This rider directs HHSC to “pursue flexibility” from the federal government to reduce Texas Medicaid 2018-2019 spending by $1 billion GR ($2.4 billion All Funds). As worded in the House Appropriations Committee bill, the rider raises concerns that it could direct or allow very large program cuts. It simply directs HHSC to identify cost savings and report changes to Medicaid and CHIP to the LBB. Before taking a vote, committee Chairman Zerwas sought to reassure members that services would not be compromised. Amendments to better clarify the intent are expected to be offered on the House floor.
The three potential reductions to Medicaid spending listed above from the House Committee bill total $1.56 billion GR. Add to that the lack of funding for projected Medicaid cost growth which may approach $2 billion GR (and which the Senate has also neglected to fund in its budget), and we could be approaching—or exceeding—the scope of cuts adopted in 2003 and 2011.
Except for one thing. Only the HHSC Cost Containment rider 36 actually directs program cuts. As discussed in a recent blog on the Senate’s original filed budget, Texas has in a number of sessions over the last 20 years short-funded Medicaid to allow for a smaller balanced budget to be passed, but guaranteeing a substantial supplemental appropriation will be required in the next session to fund the final months of Medicaid (costs are currently running around $1.5 billion GR a month).
When budget writers do not direct the Medicaid agency to make a program, eligibility, or benefit cut to reduce spending to meet the state funding written into the budget, then the under-funding does not have to result in reduced eligibility or services for Texans on Medicaid. The Legislature can fill the gap in the next session. But they can only fill that gap if the state has the revenues available. Without revenues to fill these gaps, cuts could be forced, and fewer Texans in need of Medicaid will be covered, and/or the children, seniors, Texans with disabilities and pregnant women served today will get fewer health care services.
We hope that the final bill adopted by the full House will quell some of these fears. But as we wait for those actions, we remain deeply concerned about the large size of the Medicaid under-funding, and worried that the gaps may become cuts that are even deeper than the failed cuts of 2003.